
Altitude Sickness Prevention: How to Stay Safe on High-Altitude Treks
Medical Disclaimer: This guide about AMS prevention is for general educational purposes only and is not a substitute for professional medical advice. Always consult a qualified physician before your high-altitude trek.
Most people who develop altitude sickness on a trek did not get unlucky. They got ahead of their body.
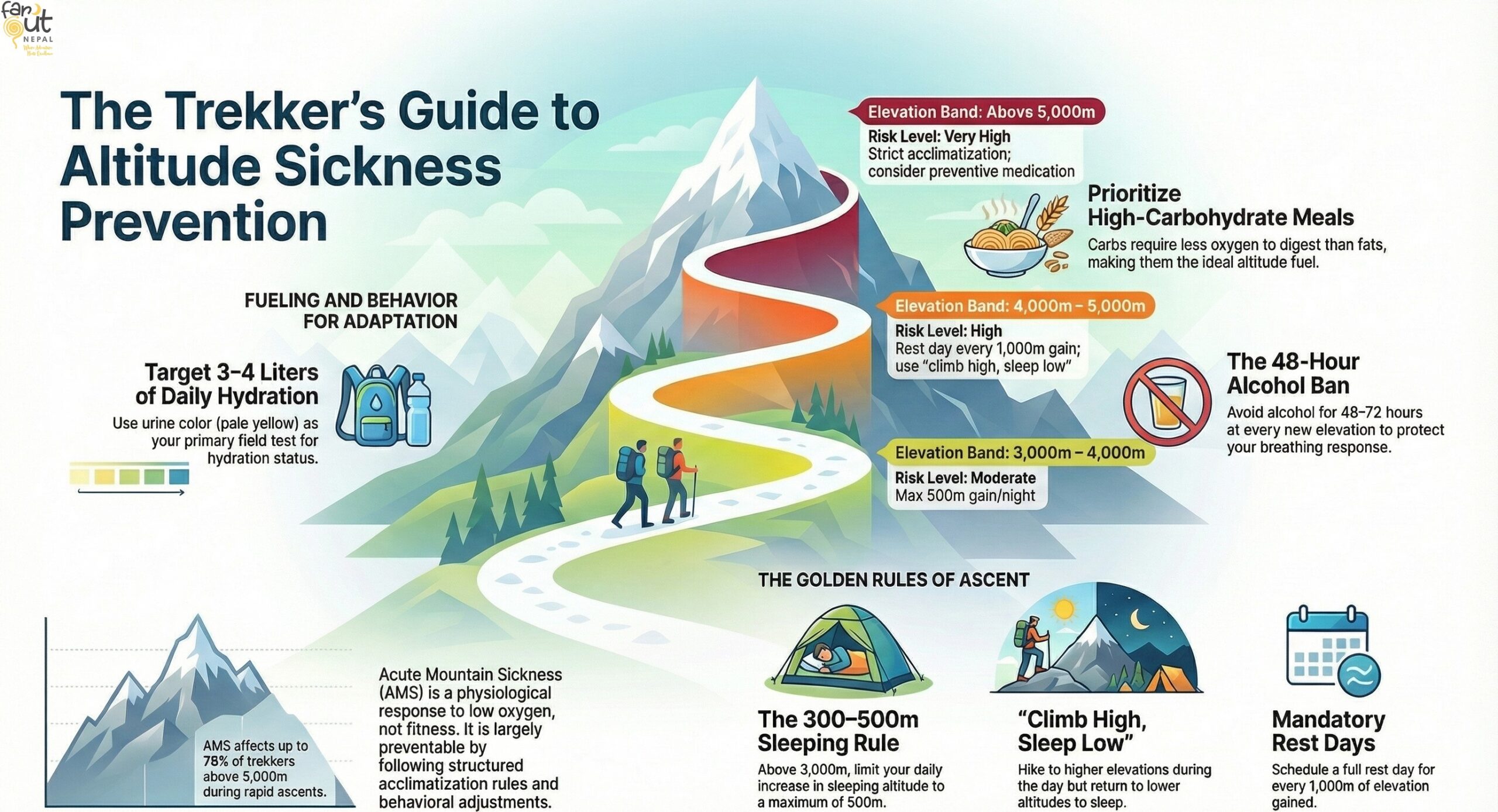
Acute Mountain Sickness (AMS) affects an estimated 25–40% of trekkers above 3,500 m, and up to 75% above 5,000 m on rapid ascent profiles. It is not a sign of weakness or low fitness. It is a physiological response to ascending faster than your body can adapt. The good news: it is largely preventable. At 3,500 m, available oxygen is roughly 65% of sea level. Your body can still adapt fully, but only if you give it time.
This guide covers everything that actually works. For a full clinical overview of AMS, HAPE, and HACE, see our complete altitude sickness guide.
The One Rule That Prevents Most Cases of AMS
Ascend gradually. Limit sleeping altitude gain to 300–500 m per night once you are above 3,000 m.
That single rule, when applied consistently, eliminates the majority of AMS risk. Everything else in this guide supports it or fills the gaps around it. The Wilderness Medical Society and CDC both cite this as the most consistently supported guideline in altitude medicine.
The companion principle: climb high, sleep low. Go for day hikes to higher elevations, followed by sleeping lower to accelerate acclimatization, while preventing overnight hypoxic stress simultaneously. This is why Namche Bazaar rest days on the EBC route include a hike up to the Everest View Hotel (3,880 m) before sleeping back at 3,440 m. It is not scenic padding; it is physiology.
Trek-Specific Acclimatization: What the Routes Actually Require
Generic advice says “go slow.” Here is what that means on some of the most popular trails.
Everest Base Camp (EBC)
The EBC route is well-designed for acclimatization when followed correctly. The mandatory rest days at Namche Bazaar (3,440 m) and Dingboche (4,360 m) are not optional stops. They are where your body does the physiological work that allows you to reach 5,364 m safely.
The most common mistake: shortening the Dingboche rest day because you feel good. Feeling fine at 4,360 m is the acclimatization working. Protect the rest days.
Annapurna Base Camp (ABC)
The ABC route has a steeper altitude gain profile than EBC and less built-in acclimatization time. Trekkers gain significant elevation quickly from Chhomrong (2,170 m) to ABC (4,130 m) in relatively few days, with limited descent options along the way.
The key mitigation: do not rush the lower sections. Time spent at Chhomrong (2,170 m) and Himalaya Hotel (2,900 m) pays dividends at ABC. A slower lower section beats a forced rest day at 3,500 m with symptoms already developing.
Manaslu Circuit
The Manaslu Circuit crosses Larkya La Pass at 5,106 m in a remote area where helicopter evacuation is far more difficult than on EBC. Rest days at Samagaun (3,530 m) and Samdo (3,875 m) are non-negotiable before even reaching the pass. The remoteness raises the stakes. So, be careful and plan accordingly.
Altitude Thresholds at a Glance
| Elevation Band | Typical Risk | Acclimatization Action Required |
| Below 2,500 m | Minimal | None |
| 2,500–3,000 m | Low–mild | Begin monitoring; no rushing |
| 3,000–4,000 m | Moderate | Max 500 m sleeping gain/night; rest days every 3rd day |
| 4,000–5,000 m | High | Rest day every 1,000 m gain; climb high, sleep low |
| Above 5,000 m | Very high | Strict acclimatization; medication consideration warranted |
Behavioural Prevention: The Habits That Move the Needle
Hydration and the Myths Around It
Target 3–4 litres of water per day at altitude. At high elevation, you lose water faster than you realise, through increased respiration rate and dry mountain air. Dehydration mimics and worsens AMS symptoms, particularly headache and fatigue.
The myth to dispel: More is not always better. Excessive water without electrolytes can cause hyponatremia, a condition that mimics AMS and can be serious. Plain water is fine; electrolyte tablets are a practical supplement on heavy days. Herbal teas in Nepal’s teahouses count toward your fluid target.
Urine colour is your simplest field test. Pale yellow is acclimatized and hydrated. Dark yellow means drink more. Clear throughout the day may mean you are overdoing it.
Alcohol: Leave It at Kathmandu
Avoid alcohol for the first 48–72 hours at every new elevation. This is not a general wellness tip, but specific physiology. Alcohol suppresses the hypoxic ventilatory response. It’s the mechanism by which your brain signals your lungs to breathe harder in low-oxygen conditions. At altitude, that mechanism is the entire acclimatization process. Blunting it during the most critical adaptation window significantly increases AMS risk.
One night of drinks at Namche before your rest day hike is not worth the next 36 hours of impaired adaptation. After your acclimatization is established at a given elevation, moderate consumption is less critical, but the first nights at each new altitude band are when it matters most.
Caffeine: More Nuanced Than You Think
Caffeine is not straightforwardly harmful at altitude. In fact, for regular coffee drinkers, stopping caffeine abruptly before a trek is a mistake. And caffeine withdrawal headache is clinically indistinguishable from an AMS headache and creates confusion at exactly the wrong moment.
The sensible approach: Maintain your normal caffeine intake. Do not dramatically increase it, as stimulants can disrupt sleep quality at altitude. But do not cut it out cold either. Nepal’s teahouses serve excellent tea and coffee. So, your morning cup is fine.
Sleep: The Underrated Prevention Tool
Most acclimatization happens during sleep. Specifically, the adjustments in ventilation, blood chemistry, and circulation that your body makes overnight. Poor sleep at altitude is both a symptom and a driver of AMS progression.
At higher elevations, Cheyne-Stokes respiration (an irregular stop-start breathing pattern) is nearly universal and disrupts sleep quality significantly. Acetazolamide reduces this substantially if you are already taking it. For those not on medication: avoid sleeping aids, alcohol, and sedatives at altitude, all of which suppress the breathing patterns your body is working hard to regulate.
Good sleep hygiene at altitude: Warm, well-ventilated room, consistent sleep schedule, and take poor sleep seriously as it can compound over days.
Overexertion: The Most Preventable Mistake
Fit trekkers are statistically just as susceptible to AMS as unfit ones. Sometimes, even more than average trekkers, because fitness breeds confidence and confidence leads to overexertion. Move at a conversational pace on ascent days. If you cannot speak comfortably while walking, slow down. On rest days, a short uphill walk and return beats complete inactivity, but it should feel easy.
Nutrition and Natural Remedies
What to Eat for Acclimatization
High-carbohydrate, lower-fat meals are physiologically sound at altitude. Carbohydrates require less oxygen per unit of energy produced than fats or proteins. This can be a real, if modest, advantage when oxygen is the limiting factor. Nepal’s dal bhat (rice, lentils, vegetables) is genuinely well-suited to altitude nutrition: high-carb, warm, easy to digest, and calorie-dense.
Practical guidance for the trail:
- Eat regularly even when your appetite drops. Reduced appetite is normal at altitude, but skipping meals impairs recovery.
- Prioritise warm, easily digestible food over heavy or fatty meals.
- Avoid large meals before sleep, which worsens the periodic breathing that disrupts rest at altitude.
Natural Remedies: What the Evidence Actually Says
This is an area where trekker culture and clinical evidence part ways. Here is an honest assessment:
Ginger — Has reasonable clinical evidence for reducing nausea, which is a common AMS symptom. It will not prevent AMS but may make mild symptoms more manageable. Ginger tea is widely available in Himalayan teahouses and is worth including.
Garlic — Traditional use in Sherpa and high-altitude communities is well-documented. Clinical evidence for AMS prevention is limited, but there is no downside to including it in meals. Garlic soup is a staple on most EBC teahouse menus.
Rhodiola rosea — An adaptogenic herb with some research interest for altitude adaptation. Early studies are inconclusive; it is not a substitute for acclimatization.
The honest summary: Natural remedies are supplements, not cures. None replaces acclimatization. Some (ginger, garlic) are worth including for comfort. None should change your itinerary decisions.
Pre-Trek Training: What Helps and What Doesn’t

Fitness does not prevent AMS: This is the most important myth to dispel. Elite athletes get AMS at the same rate as casual trekkers. Neither prior success at altitude nor cardiovascular conditioning acclimatizes your respiratory system to hypoxia. What training does is it makes the trek less exhausting, which reduces the risk.
Practical pre-trek preparation (8–12 weeks out):
- Cardiovascular base: Regular aerobic exercise, such as hiking, stair climbing, cycling, etc. Three to four sessions per week at sustained moderate intensity is the best.
- Load-bearing practice: Train with a loaded pack on hills or stairs. Descent conditioning and ankle stability matter as much as uphill strength.
- Altitude exposure if accessible: A weekend at 2,000–3,000 m in the weeks before departure is genuinely useful, though not essential.
- Sleep: Consistent quality sleep in the build-up period supports recovery capacity on the trail.
Preventive Medication
Acetazolamide (Diamox) is the most commonly prescribed preventive medication for AMS. Taken the day before ascending above 3,000 m, it compresses the acclimatization process and reduces risk, particularly for trekkers with prior AMS history or compressed itineraries. It supports the prevention principles above; it does not replace them.
For dosage, side effects, and the CDC risk framework, see our altitude sickness medication guide.
Prevention Checklist
Before you leave:
- Book an itinerary with acclimatization days built in
- See a travel medicine physician 4–6 weeks out
- Discuss acetazolamide if indicated
- Complete 8–12 weeks of cardio conditioning
- Pack electrolyte tablets and a reliable hydration system
On the trail:
- Max 300–500 m sleeping altitude gain per night above 3,000 m
- Never ascend with active AMS symptoms
- 3–4 litres of water daily, monitor urine colour
- No alcohol for 48–72 hours at each new elevation
- Maintain normal caffeine intake
- High-carb warm meals; avoid heavy meals before sleep
- Rest days should include a short uphill walk, not full inactivity
- Know the early symptoms: headache, nausea, fatigue, disturbed sleep
The Bottom Line for AMS Prevention
Altitude sickness is not a lottery. The AMS symptoms follow predictable patterns and respond to predictable interventions. The trekkers who reach Everest Base Camp, Annapurna Base Camp, or the top of Larkya La without incident are not usually tougher or fitter, but are better prepared and better paced. Plan your ascent. Protect your rest days. Trust the process.
Planning a high-altitude trek in Nepal? Our itineraries are designed with acclimatisation built into every elevation gain — not as an afterthought, but as the foundation of a safe and successful trek. → Browse our Nepal trekking trips


