
Altitude Sickness: An Overview of Acute Mountain Sickness (AMS)
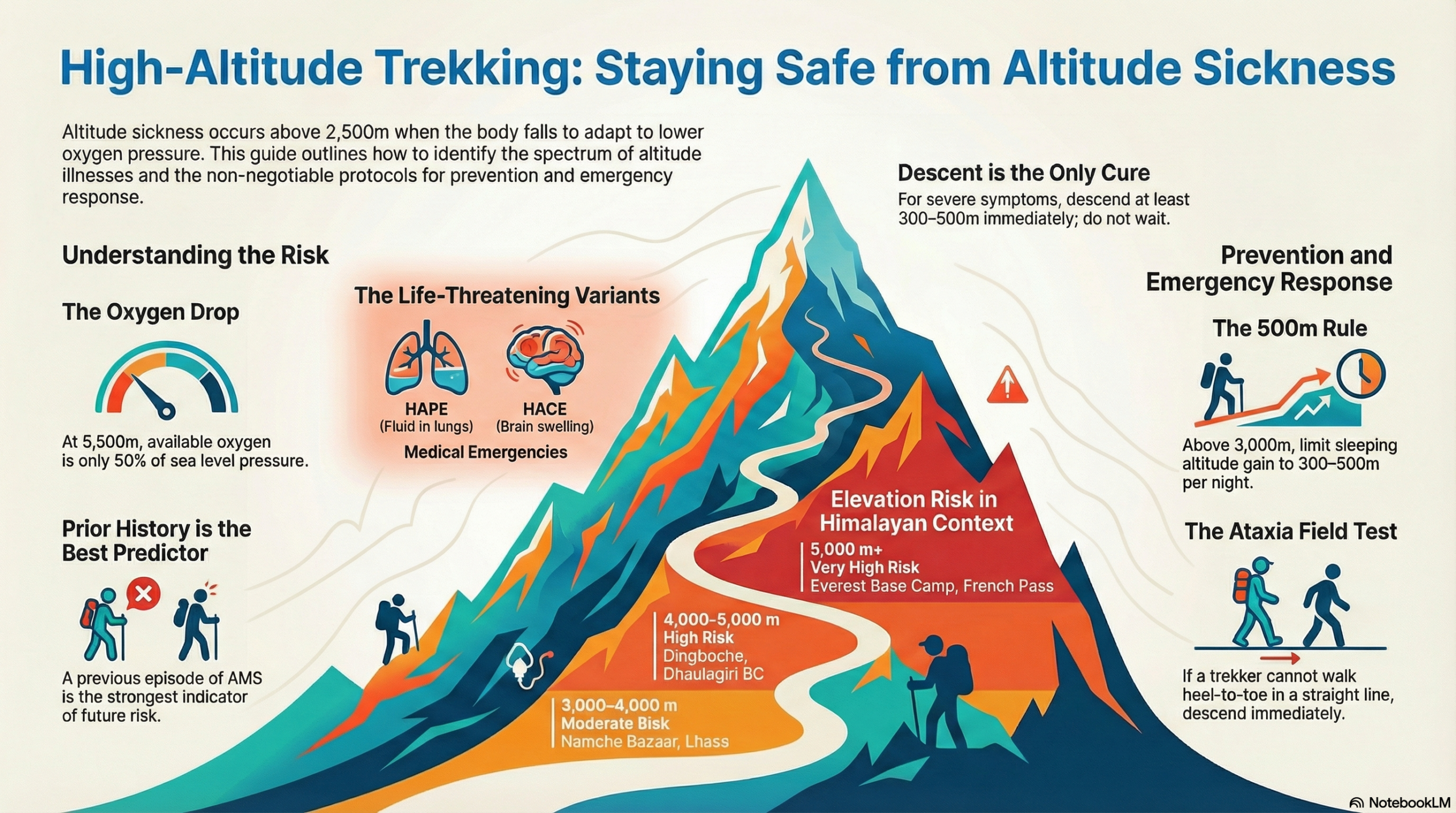
Altitude sickness or Acute Mountain Sickness (AMS) is a physiological response to the decrease in oxygen availability at high elevations, typically occurring above 2,500 m (8,200 ft). It develops when the body ascends faster than it can adapt to the drop in oxygen partial pressure, placing stress on the brain, lungs, and cardiovascular system.
Most trekkers experience some degree of AMS above 3,000 m. On popular Himalayan routes, the risk escalates significantly above 3,500 m and reaches its highest point above 5,000 m, where oxygen availability is roughly 50% of sea level.
AMS is the most common form, but altitude illness also includes two serious, life-threatening conditions: High-Altitude Pulmonary Oedema (HAPE) and High-Altitude Cerebral Oedema (HACE). Both require immediate descent and emergency care.
Note: This guide is intended as general educational content for trekkers planning high-altitude travel. It is not medical advice. Individual responses to altitude vary significantly, and nothing here should substitute for professional guidance from a qualified physician or certified mountain guide. If you or someone in your group is experiencing severe symptoms at altitude, descend immediately and seek professional help.
Why Does Altitude Sickness Happen?
As elevation increases, the atmospheric (barometric) pressure drops. Lower pressure means fewer oxygen molecules per breath, even though the percentage of oxygen in the air remains constant at 21%. At 3,500 m, available oxygen is approximately 65% of sea level. At 5,500 m, it falls to around 50%.
When the body ascends rapidly, it cannot compensate quickly enough. The physiological responses, like increased breathing rate, elevated heart rate, changes in blood chemistry, etc., take from days to weeks for stabilisation. If you ascend faster than this window allows, then AMS follows.
Individual Risk Factors
There is no reliable predictor of who will develop altitude sickness. Physical fitness offers minimal protection. Even the elite athletes are just as susceptible as casual trekkers. Key risk factors include:
- Rapid ascent rate above 3,000 m
- Sleeping at a new high altitude without adequate acclimatisation days
- Dehydration and overexertion during ascent
- Residence at or near sea level
- Genetic susceptibility (not yet predictable through standard testing)
- Age: Children and young adults may be at slightly higher risk in some studies, though the effect largely disappears when the ascent rate is controlled for
Altitude Risk Bands in the Himalayan Context
| Elevation | Risk Level | Reference Points |
| Below 2,500 m | Minimal | Kathmandu (1,400 m), Pokhara (820 m), Paro (2,200 m) |
| 2,500–3,000 m | Low–Mild | Lukla (2,860 m), Shana/Bhutan trail start |
| 3,000–4,000 m | Moderate | Namche Bazaar (3,440 m), Lhasa (3,656 m), Jangothang (4,080 m) |
| 4,000–5,000 m | High | Dingboche (4,360 m), Dhaulagiri BC (4,740 m), Namtso Lake (4,718 m) |
| 5,000 m+ | Very High | EBC (5,364 m), Kala Patthar (5,545 m), French Pass (5,360 m), Rinchen Zoe La (5,320 m) |
How AMS Risk Compounds
No single factor determines whether you will develop altitude sickness. The variables that matter most are your prior history with AMS, how fast you ascend, and the altitude you are targeting. A trekker with no prior AMS history ascending gradually to 4,000 m sits in a fundamentally different risk category than someone with a previous AMS episode pushing rapidly above 5,000 m.

These three variables are the foundation, but additional factors can push any row up one level: dehydration, alcohol consumption in the first 48–72 hours at a new elevation, overexertion on ascent days, and arriving at altitude with a pre-existing respiratory illness, all of which meaningfully increase risk beyond what the table reflects.
One finding worth noting: Prior AMS history is the strongest individual predictor by a significant margin. If you have experienced AMS before, assume you will experience it again unless your ascent profile is carefully managed. A previous episode does not confer any immunity or tolerance.
Types of High-Altitude Illness
Altitude illness exists on a spectrum. AMS is common and manageable with rest. HAPE and HACE are critical medical emergencies. Understanding their difference is the most critical safety knowledge for any high-altitude trekker.
Acute Mountain Sickness (AMS)
AMS is the most prevalent form, affecting an estimated 25–50% of trekkers above 3,500 m and up to 75% at elevations above 5,000 m on trekking routes, with rates climbing higher on rapid, unmanaged ascent profiles. It typically develops within 6–12 hours of reaching a new altitude. The defining feature is a headache, combined with at least one other symptom such as fatigue, nausea, or dizziness. AMS is graded using the Lake Louise Score (LLS), where a score of 3 or above (with headache present) indicates AMS. Moderate-to-severe scores are a clear signal to stop ascending.
High-Altitude Pulmonary Edema (HAPE)
HAPE involves fluid accumulation in the lungs and is the leading cause of altitude-related death among trekkers. It most often develops 2–4 days after arriving at altitude, more commonly on the second night at a given elevation than the first. Early signs include reduced exercise tolerance and a dry cough. As it progresses, breathlessness at rest and a productive cough with pink or frothy sputum develop. HAPE can deteriorate within hours. The occurrence is estimated at 1–6% of high-altitude travellers, depending on ascent rate and elevation profile.
HAPE is a medical emergency. If breathlessness occurs at rest or a persistent cough develops with pink or frothy sputum, immediate descent is required. Do not wait further.
High-Altitude Cerebral Edema (HACE)
HACE is the most severe form of altitude illness, involving swelling of the brain. It typically follows severe, untreated AMS. The hallmark symptom is ataxia: the loss of coordination or inability to walk a straight line. Confusion, altered consciousness, and severe headache unresponsive to pain relief are warning signs. HACE can progress to coma within 24 hours.
Incidence is estimated at less than 1% of high-altitude travellers, but mortality is high without rapid descent.
HACE is a life-threatening emergency. Any trekker showing confusion, extreme drowsiness, or loss of coordination at altitude must descend immediately. This is not a condition to monitor, but an emergency to act on.
| Feature | AMS | HAPE | HACE |
| Primary Organ | Brain/Systemic (Mild) | Lungs | Brain (Severe) |
| Severity | Common; manageable with rest | Emergency. The leading cause of death | Emergency; most severe form |
| Defining Sign | Headache + Nausea/Fatigue | Breathlessness at rest & pink/frothy spit | Ataxia (loss of coordination) & confusion |
| Urgency | Stop ascent; rest | Immediate descent is mandatory | Immediate descent is mandatory |
Symptoms of Altitude Sickness
Symptoms range from mild discomfort to a life-threatening emergency. Recognising where on this spectrum a person sits is the most important safety skill for any high-altitude trekker.
Mild AMS
Symptoms typically appear 6–12 hours after reaching altitude and may resolve with rest at the same elevation:
- Headache (dull or throbbing, often worse at night, defining indication)
- Fatigue and weakness
- Reduced appetite
- Difficulty sleeping, including irregular breathing during sleep
- Mild dizziness
Moderate AMS
If mild symptoms persist or worsen after 24 hours, or if the following develop, do not ascend further:
- Worsening headache not relieved by standard pain relief
- Nausea and vomiting
- Increasing fatigue and weakness
- Reduced urine output
- Shortness of breath on mild exertion
Severe AMS / Early HAPE or HACE
These are emergency warning signs. The trekker should not be left alone, and descent should begin immediately:
- Breathlessness at rest or with minimal movement
- Persistent dry or wet cough, especially with pink or frothy sputum
- Loss of coordination and inability to walk in a straight line (ataxia)
- Confusion, disorientation, or unusual behaviour
- Severe headache unresponsive to medication
- Extreme fatigue. Patient is unable to stand without assistance
Field test for ataxia: Ask the trekker to walk heel-to-toe in a straight line. If they cannot do this, treat it as a severe symptom and arrange descent.
How to Prevent Altitude Sickness: Overview
The single most effective prevention is controlled, gradual ascent. No supplement, food, or preparation can replace the body’s need for time to acclimatise. The following principles apply across all high-altitude treks:
- Ascend gradually. Above 3,000 m, limit sleeping altitude gain to 300–500 m per night. This is the most consistently supported guideline in wilderness medicine.
- Climb high, sleep low. Day hikes to higher elevations, followed by descending to sleep at lower altitudes, accelerate acclimatisation. This principle is built into most well-designed Himalayan itineraries.
- Build in acclimatisation days. Rest days at key elevations, like Namche Bazaar (3,440 m) and Dingboche (4,360 m) on the EBC route, are not optional padding. Skipping them significantly increases AMS risk.
- Stay hydrated. Aim for 3–4 litres of water per day at altitude. Dehydration worsens AMS symptoms and is common due to increased respiratory water loss in dry mountain air.
- Avoid alcohol and sedatives. Both suppress respiratory drive during sleep, impairing the body’s natural ventilatory response to altitude. This effect is most significant in the first 48–72 hours at a new elevation.
- Do not ascend with symptoms. If any AMS symptoms are present, rest at the current altitude until they fully resolve. This rule applies regardless of itinerary pressures.
For a full prevention guide, including acclimatisation schedules, training recommendations, and the role of medications, see our complete altitude sickness prevention guide.
Treatment of Altitude Sickness
Treatment depends on severity. The underlying principle across all levels is the same: do not ascend until symptoms resolve, and descend if they worsen or fail to improve.
Mild AMS: Rest at the current altitude. Do not ascend. Most mild AMS resolves within 12–48 hours with adequate rest and hydration. Ibuprofen (commonly used at 400 mg) has demonstrated efficacy for headache relief in clinical studies but does not treat the underlying cause.
Moderate AMS: Stop all ascent. If symptoms do not improve after 24 hours of rest, descend 300–500 m. Even a modest descent often produces rapid symptom relief. Supplemental oxygen, where available, can provide temporary relief.
Severe AMS, HAPE, or HACE: Descent is the only definitive treatment. There is no alternative. Descend immediately (at minimum 300–500 m), more if logistics allow
- Do not wait for morning or better weather if the trekker’s condition is deteriorating
- Supplemental oxygen reduces symptoms during descent but does not replace descent
- Portable hyperbaric chambers (e.g., Gamow bags) can simulate descent in emergencies and are carried by rescue teams on major Himalayan routes
Do not self-medicate based on information in this guide. Always consult a physician before your trek.
Medication options, including acetazolamide (Diamox) and dexamethasone, are covered in detail in our medication guide.
Natural Remedies: What the Evidence Says
Various foods and supplements are cited as altitude sickness aids, particularly in Himalayan and Andean cultures. The evidence for most is limited, and none replace acclimatisation.
- Ginger: some evidence for reducing nausea associated with AMS, but no demonstrated effect on core AMS progression
- Garlic: traditional use in Himalayan communities; no robust clinical evidence for altitude illness prevention
- High-carbohydrate diet: Carbohydrates require less oxygen to metabolise than fats or proteins, which may provide a marginal support for energy production at altitude. The effect is modest but supported by general physiology.
- Coca leaves / tea: widely used in South American high-altitude communities; evidence is anecdotal, and use is culturally and legally context-specific
Hydration, adequate sleep, and a conservative ascent profile remain the only interventions with consistent evidence.
Helicopter Evacuation Considerations
On major trekking routes in Nepal, helicopter evacuation is available in clear weather conditions. However:
- Flights depend on visibility and wind
- Patients may need to be moved to a landing zone
- Insurance verification or payment guarantee is required before dispatch
Remote circuits such as Manaslu or Dhaulagiri may involve staged evacuation due to terrain and weather constraints.
Evacuation is a logistical process, not an instant solution. Early decision-making significantly improves outcomes.
The Safety Hierarchy
Altitude emergency management follows a clear progression:
- Stop ascent
- Rest and reassess
- Descend if symptoms persist
- Evacuate if severe symptoms develop
When uncertain, descend. Altitude illness responds to elevation loss. Delay increases risk. A well-planned trek with built-in acclimatisation, experienced leadership, and a defined evacuation protocol reduces severe altitude complications from likely to unlikely.
Altitude Sickness on Popular Himalayan Treks
Nepal’s, Tibet’s, and Bhutan’s major trekking routes all pass through significant altitude bands. Risk profiles differ by route based on maximum elevation, rate of ascent, and availability of acclimatisation days.
| Trek or Region | Maximum Elevation (m) | Maximum Sleeping Altitude (m) | AMS Risk Level | Critical Acclimatisation Points | Key High-Altitude points | Route Specific Challenges |
| Everest Base Camp (Nepal) | 5,545 m | 5,364 m | Very High | Namche Bazaar (3,440 m), Dingboche (4,360 m) | Kala Patthar (5,545 m), Everest View Hotel (3,880 m) |
|
| Dhaulagiri Circuit (Nepal) | 5,360 m | 5,050 m | Very High | Italian Base Camp (3,660 m), Glacier Camp (4,200 m), Dhaulagiri Base Camp (4,740 m) | French Pass (5,360 m), Dhampus Pass (5,240 m) |
|
| Snowman Trek (Bhutan) | 5,320 m | Above 4,000 m | Very High / Compounding | Not in source | Rinchen Zoe La (5,320 m) |
|
| Lhasa and Beyond (Tibet) | 5,200 m | 5,200 m | Very High | Lhasa (3,656 m) | Everest North Base Camp (5,200 m), Rongbuk Monastery (5,100 m) |
|
| Manaslu Circuit (Nepal) | 5,106 m | 5,100 m | High to Very High | Dharmasala (4,460 m) | Larkya La Pass (5,106 m) |
|
| Langtang Valley (Nepal) | 4,984 m | 3,870 m | Moderate to High | Kyanjin Gompa (3,870 m) | Tserko Ri viewpoint (4,984 m) |
|
| Jomolhari Trek (Bhutan) | 4,930 m | 4,080 m | Moderate to High | Jangothang (4,080 m) | Yalila Pass (4,930 m) |
|
| Annapurna Base Camp (Nepal) | 4,130 m | 4,130 m | Moderate to High | Chhomrong (2,170 m) | Annapurna Base Camp (4,130 m) |
|
In Conclusion…
Altitude sickness is the single most important health risk on any high-altitude trek. Thankfully, it is also highly manageable with the right knowledge and pacing. Understanding the symptoms, respecting gradual acclimatization, and responding early to warning signs are what allow trekkers to safely reach destinations like Everest Base Camp, Annapurna Base Camp, and beyond. The mountains reward patience, not speed. When you prioritize acclimatization over ambition, you dramatically increase both your safety and your chances of success.
Planning a high-altitude trek?
Explore our carefully designed itineraries with built-in acclimatisation days and expert guidance to help you trek safely and confidently👉 Check out the Trips


