Tag: altitude sickness
Altitude Sickness Medication: Diamox, Dosage & What Actually Works

Introduction: Diamox or Acetazolamide
Picture this: You have booked your first EBC trek. You are ready to fly to Kathmandu, take a flight to Lukla, and spend sixteen days in the mountains. As you do some research, someone in a forum mentions Diamox, and suddenly, you are digging medical PDFs, wondering whether you actually need it.
Here is the short answer: Acetazolamide ( or Diamox) is the most commonly prescribed medication for altitude sickness. It is not a magic pill, though. Whether you need it depends almost entirely on your trek profile, your personal history, and the itinerary you are following.
Medical Disclaimer: This guide is for general educational purposes only and is not a substitute for professional medical advice. Always consult a qualified physician before taking any medication for altitude sickness.
What Is the Best Medication for Altitude Sickness?
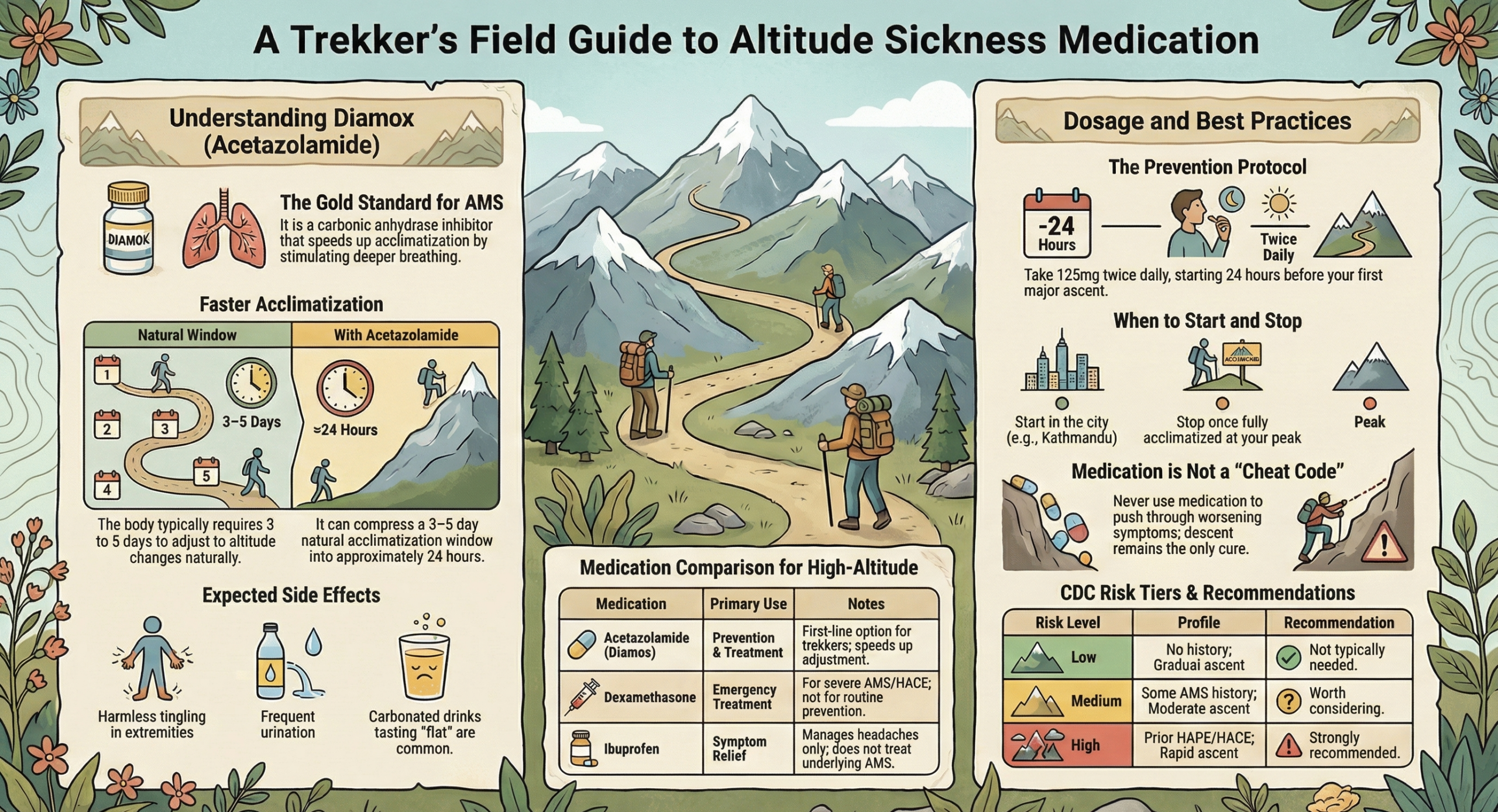
The drug of choice is always acetazolamide, sold under the brand name Diamox. It stimulates faster, deeper breathing, which accelerates the body’s acclimatization process rather than just masking symptoms like headache.
Acetazolamide may be the most prescribed, but it is not the only drug used in altitude illness management.
| Medication | Primary Use | When It’s Used | Notes |
| Acetazolamide (Diamox) | Prevention + treatment of AMS | Before and during ascent | First-line option; commonly prescribed |
| Dexamethasone | Emergency treatment of severe AMS, HACE | Serious symptoms; evacuation situations | A corticosteroid — not for routine prevention; carried by guides and rescue teams |
| Ibuprofen | Headache relief in mild AMS | Symptom management | Treats headache only; does not address underlying AMS |
| Nifedipine | Emergency treatment of HAPE | Life-threatening lung fluid accumulation | Specialist use; not a trekker’s self-medication option |
The important distinction: Dexamethasone and Nifedipine are emergency medications. They are carried by experienced guides and rescue teams on routes like EBC and Manaslu for life-threatening situations. They’re not alternatives to acetazolamide for everyday prevention.
Ibuprofen (typically 400 mg) is useful for managing headache in mild AMS and is worth carrying regardless. It does not treat the cause, but it can make the acclimatization window more bearable.
How Diamox Actually Works
Your body’s adjustment to altitude is essentially a breathing problem. At 5,000 m, every breath delivers roughly half the oxygen it would at sea level. To compensate, your body needs to breathe more, but the signal chain that triggers this response takes days to calibrate.
Acetazolamide is a carbonic anhydrase inhibitor. In plain terms, it nudges your kidneys to release bicarbonate, which slightly acidifies your blood. That acidification tells your brain to breathe harder. More oxygen in, faster acclimatization.
According to the CDC Yellow Book (2026 edition), the ventilatory acclimatization that normally takes 3–5 days is compressed to approximately one day with acetazolamide. That is a meaningful difference on a trek where every acclimatization day counts.
It also helps with something most trekkers do not expect: sleep. Above around 2,700 m, periodic irregular breathing becomes nearly universal and wrecks your rest at altitude. Acetazolamide improves nocturnal oxygen saturation and reduces it significantly, which means you wake up feeling less wrecked the morning before a big climb.
What it does not do is allow you to cheat the mountain. It cannot prevent HAPE or HACE if you are ascending recklessly. It does not eliminate AMS risk, but reduces it. And it will not save you from a bad itinerary.
Diamox Dosage for Altitude Sickness
Based on current wilderness medicine guidelines and the CDC Yellow Book (2026):
Important: These are standard reference dosages. Your physician may adjust based on your weight, health history, and risk profile. Always follow your prescribing doctor’s specific guidance.
For Prevention
The standard prevention dose is 125 mg twice daily, starting the day before you ascend above 3,000 m and continuing for the first two days at altitude, longer if you keep ascending.
| Use | Dose | Frequency |
| Standard | 125 mg | Twice daily |
| Body weight >100 kg | 250 mg | Twice daily |
The 125 mg dose is increasingly preferred over the older 250 mg standard because it produces far fewer side effects while maintaining effectiveness. The CDC specifically flags 250 mg for trekkers over 100 kg.
For Treatment
If AMS symptoms appear, the commonly used treatment dose is 250 mg twice daily. This is taken alongside rest at the same altitude, not as an enhancement to push higher.
| Use | Dose | Frequency |
| Treatment of AMS | 250 mg | Twice daily |
One important note: If symptoms are worsening despite medication, descent is the only answer. Diamox is not a substitute for going down.
How to Take Diamox on a Nepal Trek
Timing is everything here, and most first-time trekkers get it slightly wrong.
Start the day before ascent. Not the morning you fly to Lukla or drive to the trailhead. For an EBC trek, that means taking acetazolamide the day before your Lukla flight, when you are still in Kathmandu. By the time you land at 2,860 m, the medication is already active.
Continue for the first 2–3 days at each new altitude band. On the EBC route, this aligns with your rest days at Namche Bazaar (3,440 m) and Dingboche (4,360 m). On the Manaslu Circuit, it applies from Samagaun onwards. On Annapurna Base Camp, the compressed profile makes the early days particularly important.
Stop once you are fully acclimatized at your highest point. No need to continue during descent as the work is done.
A few practical things that matter on the trail:
- Take it with food. An empty stomach makes nausea more likely.
- Drink more water than you think you need. Acetazolamide is a mild diuretic, and dehydration is already a risk at altitude.
- Avoid alcohol for the first 48–72 hours at any new elevation. It suppresses the respiratory drive that the medication is trying to stimulate and independently increases AMS risk.
Do You Actually Need Diamox?
The CDC Yellow Book (2026) categorizes AMS risk into three tiers based on your altitude illness history, your sleeping altitude on day one, and your rate of ascent:
| Risk Level | Your Profile | Recommendation |
| Low | No AMS history · sleeping altitude <2,750 m on day 1 · ascent ≤500 m/night | Not typically needed |
| Medium | Some AMS history · sleeping 2,750–3,400 m on day 1 · faster ascent with rest days | Worth considering |
| High | HAPE/HACE history · sleeping >3,400 m on day 1 · rapid ascent without rest days | Strongly recommended |
The reality on most Himalayan treks: you land at Lukla (2,860 m) and reach Namche (3,440 m) within two days. That puts most trekkers squarely in the “Medium” category from day one, regardless of fitness level.
You should seriously consider acetazolamide if:
- You have had AMS before on any previous trek. Prior history is the strongest predictor of future AMS
- Your itinerary is compressed with fewer rest days than standard
- You are heading above 4,000 m with limited experience at altitude
- You are flying directly into high altitude (common on Tibet itineraries as Lhasa sits at 3,656 m)
You may not need it if:
- You are on a well-paced itinerary with proper acclimatization days built in
- You have completed similar-altitude treks before without symptoms
- Your travel medicine physician has assessed your risk as low based on your profile
The honest answer for most people planning Everest Base Camp is that it is worth the conversation with your doctor. Acetazolamide is inexpensive, widely available on prescription, and the cost of the conversation is zero.
Side Effects of Diamox: What to Actually Expect
Diamox has a reputation that puts people off. Here is what is actually going on.
Tingling in your hands, feet, and face: This is the most common side effect and the one that surprises people most. It starts a few hours after your first dose and continues throughout the course. It is harmless. If you are not experiencing it at all, it may be a sign that the medication is not at a full therapeutic level.
More bathroom trips: Acetazolamide is mildly diuretic. You will urinate more, especially in the first day or two. On a trek, this mostly means planning on long days between lodges.
Your beer tastes weird: Specifically, carbonated drinks taste flat or metallic. The enzyme that normally helps you taste carbonation is the same one that acetazolamide inhibits. Your Everest brew at Namche will taste off. This is a good sign that the medication is working.
Mild nausea: Some people experience this, almost always on an empty stomach. Food fixes it.
If you develop a skin rash, hives, or any sign of an allergic reaction, stop immediately and seek medical attention.
Who Should Avoid Diamox?
Acetazolamide is not appropriate for everyone. Your physician will screen for these, but you should know them before your consultation.
Sulfonamide (sulfa) allergy: Acetazolamide is chemically related to sulfonamide antibiotics. People with a documented sulfa allergy may react to it. This is the most significant contraindication. If you have had a reaction to sulfa drugs, flag it to your doctor before they prescribe acetazolamide.
Kidney disease or kidney stones: Acetazolamide affects how the kidneys handle bicarbonate and may increase the risk of stone formation. Anyone with a history of kidney issues should discuss this carefully with their physician.
Pregnancy: Acetazolamide is generally not recommended during pregnancy. The risk-benefit calculation at altitude is a conversation for your obstetrician.
Certain medications: It can interact with some diuretics, lithium, and other drugs. Disclose your complete medication list to your prescribing doctor.
This is precisely why the pre-trek physician consultation is not optional if you are considering medication. It takes fifteen minutes and eliminates guesswork.
Medication vs. Acclimatization: The Most Important Thing
Medication supports acclimatization. It does not replace it.
The trekkers who get into serious trouble at altitude are not usually the ones who forgot their Diamox. They are the ones who skipped the Namche rest day because they felt fine, pushed through a mild headache at Dingboche, and treated medication as a green light to move faster.
No dose of acetazolamide makes a compressed itinerary safe. The rules still apply:
- No more than 300–500 m of sleeping altitude gain per night above 3,000 m.
- Rest days at Namche Bazaar and Dingboche on the EBC routes. These are not optional extras.
- Never ascend with active AMS symptoms, regardless of what is in your pack.
Acetazolamide gives your body a better chance. The itinerary gives it the time. You need both.
For acclimatization schedules, route-specific risk profiles, and how to read early symptoms on the trail, see our complete altitude sickness guide.
Quick Reference
| Question | Answer |
| Best medication for altitude sickness | Acetazolamide (Diamox) |
| Standard prevention dose | 125 mg twice daily (250 mg if >100 kg) |
| When to start | The day before ascending above 3,000 m |
| Treatment dose | 250 mg twice daily |
| Main side effects | Tingling, frequent urination, flat taste in carbonated drinks |
| Sulfa allergy + Diamox | Not an automatic contraindication — discuss with your doctor |
| Does it replace acclimatization? | No. Never. |
So, Should You Take Diamox?
Acetazolamide is a well-studied, commonly prescribed, and genuinely useful tool for trekkers heading into high altitudes. If taken at the right dose & started at the right time, alongside a sensible ascent profile, it meaningfully reduces AMS risk and makes the acclimatization window more manageable.
But it is exactly that: a tool. The mountains do not care what is in your pack. They respond to patience, preparation, and the willingness to turn around when the situation calls for it. Medication just helps your body keep up.
If you are planning a high-altitude route, always see a travel medicine physician at least four to six weeks before departure. If you’re wondering how to detect signs and symptoms of AMS, check out our guide on AMS signs and symptoms.
Planning a high-altitude trek in Nepal? Explore our itineraries: built with acclimatisation days, experienced guides, and safety protocols designed for high-altitude terrain. 👉 Browse our Nepal trekking trips
Altitude Sickness (AMS) Symptoms: Early Signs, Severity Levels & When to Worry

Introduction
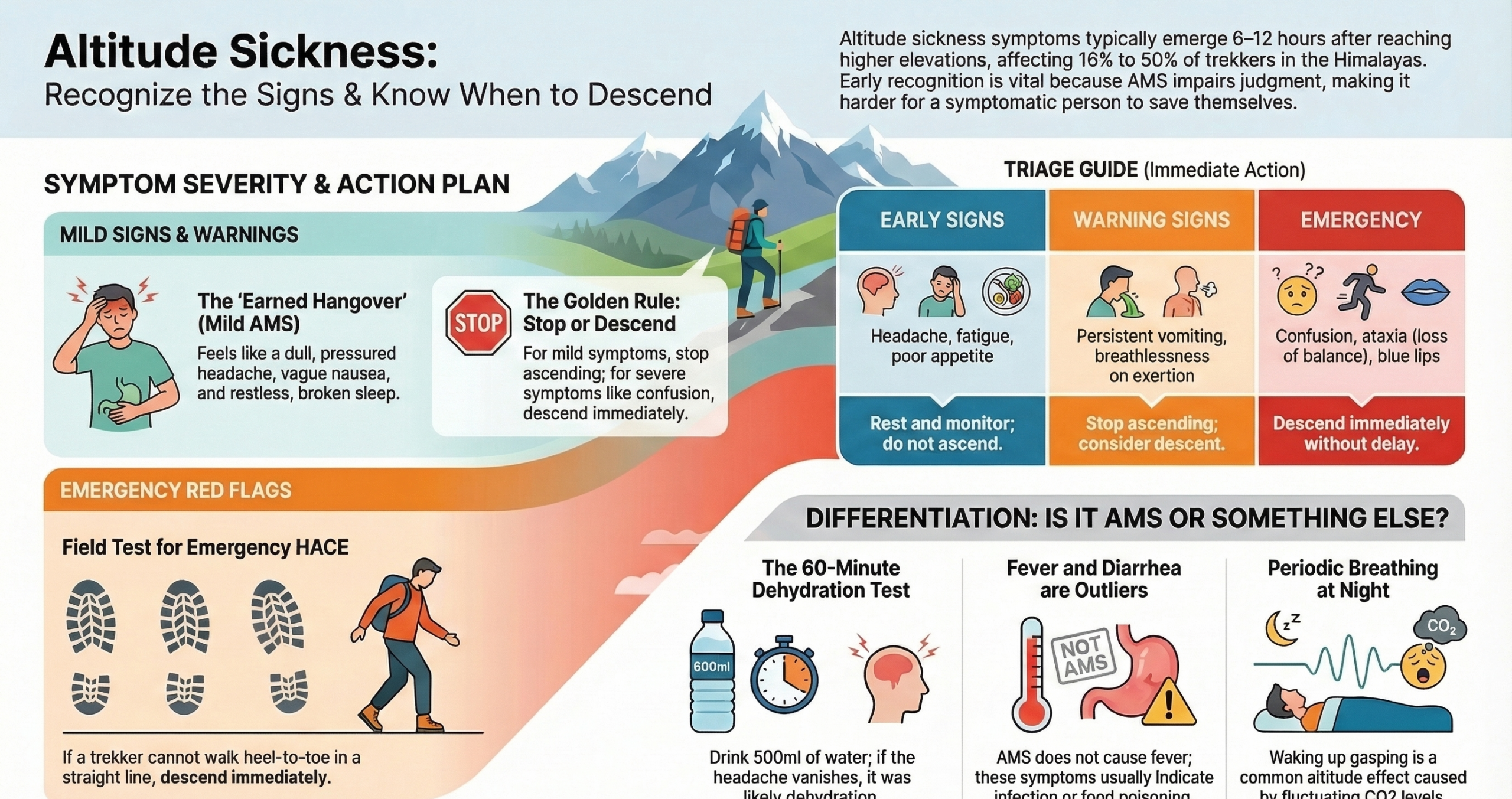
Altitude sickness symptoms usually begin to appear within 6–12 hours of reaching higher elevations. These symptoms typically range from mild headaches and fatigue to serious conditions affecting the lungs and brain. Studies in the Himalayas show AMS rates ranging from 16% to over 50%, depending on altitude and ascent speed.
This makes it one of the most common medical concerns for trekkers. Recognizing symptoms early and understanding what they actually mean is what keeps a great trek from becoming a medical emergency.
What Does Altitude Sickness Feel Like?
Most people expect altitude sickness to announce itself clearly. It rarely does and sneaks in quietly. The most honest description? It feels like a hangover you didn’t earn.
A dull, pressured headache that sits behind your eyes and wraps around your skull. A vague nausea that makes you want to vomit after smelling anything. A night of broken, restless sleep that leaves you more exhausted than when you went to bed.
What catches trekkers off guard is the subtlety. Initially, you feel off but not dramatically unwell. Many dismiss it as trail tiredness, a bad night’s sleep, or yesterday’s exertion. That dismissal is exactly where AMS gets dangerous.
The experience varies more than most expect. Some people feel genuinely terrible at mild AMS. Others feel only a little more tired. Fitness level doesn’t protect you, while experienced trekkers who lead the group on day one sometimes struggle most by day three. There is no reliable way to predict individual susceptibility in advance.
Early Signs of Altitude Sickness
The following symptoms typically appear first, often within hours of arriving at a new elevation:
- Headache: The defining symptom; throbbing or pressure-type, often worsening overnight
- Fatigue: Disproportionate tiredness that rest doesn’t fully relieve
- Loss of appetite: Food becomes unappealing, not just less enjoyable
- Mild dizziness: Lightheadedness, nausea (especially when standing or moving quickly)
- Sleep disturbance: Difficulty staying asleep, waking repeatedly, and feeling unrefreshed in the morning
A headache alone at altitude is classified as a high-altitude headache (HAH) and is extremely common. It becomes AMS when accompanied by at least one other symptom: nausea, fatigue, or dizziness. This combined symptom severity can reach a clinical threshold, which can be defined by the Lake Louise Scoring System.
If you wake up with a headache and no appetite after your first night at a new elevation, that combination deserves attention, not dismissal.
Altitude Sickness Symptoms by Severity
Mild Symptoms (Early AMS)
AMS is rare below 2,500m. Above 4,500m (which is the elevation of many popular Himalayan treks), more than half of the trekkers may be affected. Mild AMS is the most common presentation and, if managed correctly, is rarely dangerous.
- Headache that responds to ibuprofen or paracetamol
- Mild fatigue
- Reduced appetite
- Slight dizziness
- Disrupted sleep
At this stage, the right move is simple. Stop ascending. Rest at the same altitude. Most mild AMS resolves within 24–48 hours with acclimatization. The mistake people consistently make is pushing their ascent because they feel “only a little off.” That is how mild progresses to other stages.
Moderate Symptoms
Moderate AMS means your body is struggling to compensate. Symptoms intensify and begin interfering with normal functioning:
- Persistent headache that doesn’t fully respond to painkillers
- Nausea, possibly with vomiting
- Significant fatigue, where basic tasks feel effortful
- Breathlessness with mild exertion
- Reduced urine output
Do not ascend further. If symptoms don’t change (improve or worsen), even after 24 hours of rest at the same altitude, descending 300–500m is the right call. This is the stage at which ignoring symptoms creates a real risk.
Severe Symptoms (Emergency Warning Signs)
Severe AMS indicates progression toward HACE (High Altitude Cerebral Edema) or HAPE (High Altitude Pulmonary Edema). Both of these are life-threatening conditions and require immediate action.
HAPE is actually the more common cause of altitude-related death and can develop without preceding AMS symptoms in some cases. HACE, if untreated, can progress to coma and death within 12–24 hours due to brain herniation.
Descend immediately. Do not wait for morning.
- Breathlessness at complete rest
- Persistent dry cough, especially with pink or frothy sputum (HAPE)
- Confusion, disorientation, or unusual behavior
- Inability to walk a straight line (ataxia). A hallmark sign of HACE
- Extreme lethargy beyond normal exhaustion
- Blue lips or fingernails (cyanosis)
A useful field test for HACE: Ask the person to walk heel-to-toe in a straight line. If they can’t, even if they could before, descend immediately.
Specific AMS Symptoms Explained
Altitude Sickness Headache
The headache of AMS isn’t random. When oxygen levels drop, the brain triggers vasodilation, where the blood vessels widen in an attempt to push more oxygenated blood to the brain tissue. This increases intracranial pressure.
But the pain itself is generated through the trigeminovascular system. This is the same nerve pathway involved in migraines, which is why an AMS headache can feel remarkably similar to a migraine.
What makes it distinct from other headaches: It typically worsens overnight, peaks in the morning, and intensifies when bending forward or lying flat. Exertion makes it worse. It often doesn’t respond well to hydration alone, which is one of the key ways to differentiate it from a dehydration headache.
If ibuprofen isn’t meaningfully reducing it after a few hours, treat that as a signal, not a nuisance.
Nausea and Loss of Appetite
Hypoxia activates the sympathetic nervous system. This is the same stress-response system behind pre-adrenaline nausea. Simultaneously, the gut is deprioritized under low-oxygen conditions. Digestion slows. Food becomes unappealing.
In early AMS, this isn’t dramatic nausea, but a persistent, low-level queasiness. Many trekkers eat mechanically but find no enjoyment in food. Vomiting typically signals moderate-to-severe AMS, and when it appears, it matters beyond discomfort. Vomiting also accelerates dehydration and can delay acclimatization.
Dizziness and Fatigue
Dizziness at altitude stems from reduced oxygen reaching the vestibular system and brain. This is also compounded by the cardiovascular effort of compensating for hypoxia. It presents as lightheadedness, which is most noticeable when standing or changing positions quickly.
Fatigue runs deeper than just the tiredness after trekking. Muscles switch to less efficient anaerobic metabolism earlier than normal. Meanwhile, the body is working hard just to maintain basic function. There’s an increase in breathing rate, elevated heart rate, and heightened sympathetic activation. All of it burns energy. Fit, experienced trekkers are often the most surprised by how profound this fatigue feels.
Sleep Disturbances at Altitude
This is the most misunderstood AMS symptom, and the one most likely to be blamed on everything except the actual cause.
When you’re sleeping at an altitude, hypoxia triggers faster breathing (hyperpnea), which drops CO₂ levels. Low CO₂ signals the brain to temporarily stop breathing (apnea). Falling oxygen level then restarts the breathing drive, and the cycle repeats.
This is called periodic breathing, sometimes referred to as Cheyne-Stokes respiration at altitude. Each cycle lasts roughly 30 seconds to 2 minutes, though at altitude these cycles tend to be shorter and more frequent than in other clinical settings.
The result: Repeated micro-awakenings, often with a gasping or startled sensation. Vivid or unsettling dreams are common. You go to bed tired and wake up more exhausted, because you technically stopped breathing dozens of times overnight.
Many trekkers blame cold air, tent noise, or a new environment. If you’re consistently waking with a jolt at a new elevation, this is why.
Symptoms That Are Often Confused with Altitude Sickness
Knowing what altitude sickness is is just as important as knowing what it is. Once you’ve ruled out dehydration, food poisoning, or a common cold, what remains needs to be taken seriously.
Can Altitude Sickness Cause Fever?
No. Fever is not a symptom of AMS or HACE. If you have a fever above 38°C at altitude, think infection first, like viral illness, respiratory infection, or something requiring medical attention beyond altitude protocol.
The exception worth knowing: Fever can appear with HAPE, which is why HAPE is sometimes initially mistaken for pneumonia. But by that point, respiratory symptoms, including breathlessness at rest and a worsening cough, are dominant and hard to miss. A fever without those classic AMS markers points strongly away from altitude sickness.
Diarrhea at Altitude: AMS or Something Else?
Diarrhea is one of the most common medical complaints among trekkers in Nepal, but it is rarely caused by altitude. AMS only causes nausea and sometimes vomiting.
What actually causes trekker diarrhea in the Himalayas is far more mundane: contaminated water, unfamiliar food, traveler’s gut bacteria, including E. coli and Giardia. This is so prevalent in the first two weeks of a Nepal trip that many trekkers incorrectly attribute it to altitude when it needs an entirely different response of rehydration and possibly antibiotics, not descent.
Fever combined with diarrhea is almost certainly not AMS. Think food poisoning or infection.
AMS vs. Dehydration
This is the most practically useful distinction to understand, because dehydration and AMS frequently co-exist and share overlapping symptoms.
Where they overlap: headache, fatigue, nausea, dizziness.
Where they differ:
- Dehydration headache typically improves within 30–60 minutes of drinking water. AMS headache does not.
- Dehydration causes dry mouth, thirst, and dark urine. These are not typical AMS features.
- Altitude itself increases fluid loss through faster, drier breathing. Many trekkers arrive genuinely dehydrated without realizing it, which can worsen AMS symptoms.
A practical field approach: Drink 500ml of water and wait 45–60 minutes. If the headache eases meaningfully, dehydration was likely the cause. If it persists or worsens, treat it as AMS and act accordingly.
How AMS Symptoms Progress If Ignored
AMS follows a quick escalation when ascent continues despite symptoms.
Hours 6–12 after ascent: A dull headache begins, but is often dismissed as trail tiredness. Mild fatigue. Slight nausea. Easy to explain away.
Night 1: The headache intensifies when lying down. Sleep is fragmented by periodic breathing. Morning reveals worse symptoms than the evening before. This is a critical signal: if you feel worse after a night of rest, acclimatization is not happening.
24–48 hours with continued ascent: Headache becomes severe and unresponsive to medication. Vomiting. Profound fatigue. Breathlessness on minimal exertion. The body is no longer compensating.
Beyond this point: The transition to HACE or HAPE can happen within hours. Confusion appears. Coordination deteriorates. Breathing becomes labored at rest. This is a medical emergency with a narrow treatment window.
One critical and underappreciated factor:
AMS impairs judgment. The very condition requiring action makes it harder to recognize that you need to act. Guides, trek partners, and pre-agreed symptom plans matter here. You should not rely solely on self-assessment when symptomatic.
When to Be Concerned About Altitude Sickness Symptoms
Here’s a sobering finding from Nepal-based research: 63% of trekkers developed AMS symptoms despite 80% having prior knowledge of the condition.
Knowing about altitude sickness does not protect you from it. It also doesn’t guarantee you’ll recognize it in yourself.
Seek descent or emergency assistance when:
- Symptoms worsen after 24 hours of rest at the same altitude
- The headache becomes severe and doesn’t respond to ibuprofen
- Breathlessness occurs at rest, not just on the trail
- Coordination or balance deteriorates
- Confusion, unusual behavior, or extreme lethargy appear
- Any symptom from the severe category above is present
The golden rule of altitude: If in doubt, descend. Dropping even 300–500m can produce a dramatic improvement within hours. Altitude is the only reliable cure for AMS, and it works fast.
Do You Need Medication for These Symptoms?
Acetazolamide (sold under the brand name Diamox) is the most widely used medication for altitude sickness prevention and treatment. It works by inducing a mild metabolic shift that stimulates deeper, more frequent breathing, essentially accelerating what acclimatization does naturally over 3–5 days into roughly one.
It also directly reduces periodic breathing during sleep, which is why many trekkers on Diamox report significantly better rest at altitude. Importantly, it doesn’t mask symptoms, but supports the body’s actual adaptation process.
Whether you need it depends on your ascent profile, personal susceptibility, and trek itinerary. For dosage, timing, and a full breakdown of how to use it properly, see our complete altitude sickness medication guide.
Quick AMS Symptom Reference
| Category | Symptoms | Action |
| Early Signs | Headache, fatigue, poor appetite, mild dizziness, broken sleep | Rest, don’t ascend, monitor closely |
| Warning Signs | Persistent headache, nausea/vomiting, breathlessness on exertion | Stop ascending, consider descent |
| Emergency Signs | Breathlessness at rest, confusion, ataxia, pink/frothy cough | Descend immediately without any delay |
So, can we manage AMS symptoms?
Altitude sickness is manageable when you catch it early. The trekkers who get into serious trouble aren’t usually the ones who didn’t know the symptoms, but the ones who recognized them and kept climbing anyway.
Understand what your body is telling you. Know what AMS is and what isn’t. And when symptoms don’t resolve with rest, descend first and investigate later.
For a complete overview of causes, risk factors, and prevention strategies, see our complete altitude sickness overview guide.
Altitude Sickness: An Overview of Acute Mountain Sickness (AMS)

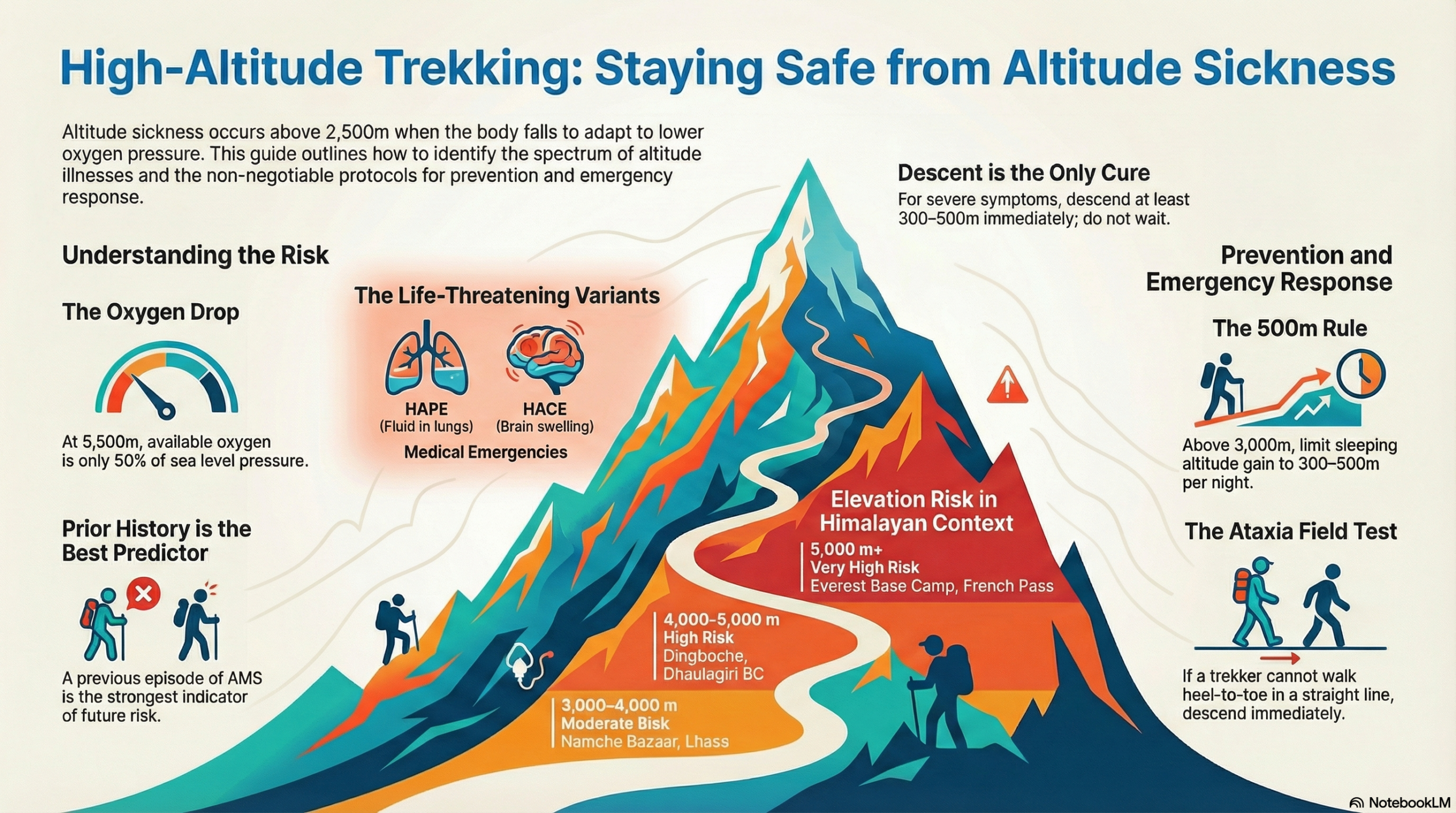
Altitude sickness or Acute Mountain Sickness (AMS) is a physiological response to the decrease in oxygen availability at high elevations, typically occurring above 2,500 m (8,200 ft). It develops when the body ascends faster than it can adapt to the drop in oxygen partial pressure, placing stress on the brain, lungs, and cardiovascular system.
Most trekkers experience some degree of AMS above 3,000 m. On popular Himalayan routes, the risk escalates significantly above 3,500 m and reaches its highest point above 5,000 m, where oxygen availability is roughly 50% of sea level.
AMS is the most common form, but altitude illness also includes two serious, life-threatening conditions: High-Altitude Pulmonary Oedema (HAPE) and High-Altitude Cerebral Oedema (HACE). Both require immediate descent and emergency care.
Note: This guide is intended as general educational content for trekkers planning high-altitude travel. It is not medical advice. Individual responses to altitude vary significantly, and nothing here should substitute for professional guidance from a qualified physician or certified mountain guide. If you or someone in your group is experiencing severe symptoms at altitude, descend immediately and seek professional help.
Why Does Altitude Sickness Happen?
As elevation increases, the atmospheric (barometric) pressure drops. Lower pressure means fewer oxygen molecules per breath, even though the percentage of oxygen in the air remains constant at 21%. At 3,500 m, available oxygen is approximately 65% of sea level. At 5,500 m, it falls to around 50%.
When the body ascends rapidly, it cannot compensate quickly enough. The physiological responses, like increased breathing rate, elevated heart rate, changes in blood chemistry, etc., take from days to weeks for stabilisation. If you ascend faster than this window allows, then AMS follows.
Individual Risk Factors
There is no reliable predictor of who will develop altitude sickness. Physical fitness offers minimal protection. Even the elite athletes are just as susceptible as casual trekkers. Key risk factors include:
- Rapid ascent rate above 3,000 m
- Sleeping at a new high altitude without adequate acclimatisation days
- Dehydration and overexertion during ascent
- Residence at or near sea level
- Genetic susceptibility (not yet predictable through standard testing)
- Age: Children and young adults may be at slightly higher risk in some studies, though the effect largely disappears when the ascent rate is controlled for
Altitude Risk Bands in the Himalayan Context
| Elevation | Risk Level | Reference Points |
| Below 2,500 m | Minimal | Kathmandu (1,400 m), Pokhara (820 m), Paro (2,200 m) |
| 2,500–3,000 m | Low–Mild | Lukla (2,860 m), Shana/Bhutan trail start |
| 3,000–4,000 m | Moderate | Namche Bazaar (3,440 m), Lhasa (3,656 m), Jangothang (4,080 m) |
| 4,000–5,000 m | High | Dingboche (4,360 m), Dhaulagiri BC (4,740 m), Namtso Lake (4,718 m) |
| 5,000 m+ | Very High | EBC (5,364 m), Kala Patthar (5,545 m), French Pass (5,360 m), Rinchen Zoe La (5,320 m) |
How AMS Risk Compounds
No single factor determines whether you will develop altitude sickness. The variables that matter most are your prior history with AMS, how fast you ascend, and the altitude you are targeting. A trekker with no prior AMS history ascending gradually to 4,000 m sits in a fundamentally different risk category than someone with a previous AMS episode pushing rapidly above 5,000 m.

These three variables are the foundation, but additional factors can push any row up one level: dehydration, alcohol consumption in the first 48–72 hours at a new elevation, overexertion on ascent days, and arriving at altitude with a pre-existing respiratory illness, all of which meaningfully increase risk beyond what the table reflects.
One finding worth noting: Prior AMS history is the strongest individual predictor by a significant margin. If you have experienced AMS before, assume you will experience it again unless your ascent profile is carefully managed. A previous episode does not confer any immunity or tolerance.
Types of High-Altitude Illness
Altitude illness exists on a spectrum. AMS is common and manageable with rest. HAPE and HACE are critical medical emergencies. Understanding their difference is the most critical safety knowledge for any high-altitude trekker.
Acute Mountain Sickness (AMS)
AMS is the most prevalent form, affecting an estimated 25–50% of trekkers above 3,500 m and up to 75% at elevations above 5,000 m on trekking routes, with rates climbing higher on rapid, unmanaged ascent profiles. It typically develops within 6–12 hours of reaching a new altitude. The defining feature is a headache, combined with at least one other symptom such as fatigue, nausea, or dizziness. AMS is graded using the Lake Louise Score (LLS), where a score of 3 or above (with headache present) indicates AMS. Moderate-to-severe scores are a clear signal to stop ascending.
High-Altitude Pulmonary Edema (HAPE)
HAPE involves fluid accumulation in the lungs and is the leading cause of altitude-related death among trekkers. It most often develops 2–4 days after arriving at altitude, more commonly on the second night at a given elevation than the first. Early signs include reduced exercise tolerance and a dry cough. As it progresses, breathlessness at rest and a productive cough with pink or frothy sputum develop. HAPE can deteriorate within hours. The occurrence is estimated at 1–6% of high-altitude travellers, depending on ascent rate and elevation profile.
HAPE is a medical emergency. If breathlessness occurs at rest or a persistent cough develops with pink or frothy sputum, immediate descent is required. Do not wait further.
High-Altitude Cerebral Edema (HACE)
HACE is the most severe form of altitude illness, involving swelling of the brain. It typically follows severe, untreated AMS. The hallmark symptom is ataxia: the loss of coordination or inability to walk a straight line. Confusion, altered consciousness, and severe headache unresponsive to pain relief are warning signs. HACE can progress to coma within 24 hours.
Incidence is estimated at less than 1% of high-altitude travellers, but mortality is high without rapid descent.
HACE is a life-threatening emergency. Any trekker showing confusion, extreme drowsiness, or loss of coordination at altitude must descend immediately. This is not a condition to monitor, but an emergency to act on.
| Feature | AMS | HAPE | HACE |
| Primary Organ | Brain/Systemic (Mild) | Lungs | Brain (Severe) |
| Severity | Common; manageable with rest | Emergency. The leading cause of death | Emergency; most severe form |
| Defining Sign | Headache + Nausea/Fatigue | Breathlessness at rest & pink/frothy spit | Ataxia (loss of coordination) & confusion |
| Urgency | Stop ascent; rest | Immediate descent is mandatory | Immediate descent is mandatory |
Symptoms of Altitude Sickness
Symptoms range from mild discomfort to a life-threatening emergency. Recognising where on this spectrum a person sits is the most important safety skill for any high-altitude trekker.
Mild AMS
Symptoms typically appear 6–12 hours after reaching altitude and may resolve with rest at the same elevation:
- Headache (dull or throbbing, often worse at night, defining indication)
- Fatigue and weakness
- Reduced appetite
- Difficulty sleeping, including irregular breathing during sleep
- Mild dizziness
Moderate AMS
If mild symptoms persist or worsen after 24 hours, or if the following develop, do not ascend further:
- Worsening headache not relieved by standard pain relief
- Nausea and vomiting
- Increasing fatigue and weakness
- Reduced urine output
- Shortness of breath on mild exertion
Severe AMS / Early HAPE or HACE
These are emergency warning signs. The trekker should not be left alone, and descent should begin immediately:
- Breathlessness at rest or with minimal movement
- Persistent dry or wet cough, especially with pink or frothy sputum
- Loss of coordination and inability to walk in a straight line (ataxia)
- Confusion, disorientation, or unusual behaviour
- Severe headache unresponsive to medication
- Extreme fatigue. Patient is unable to stand without assistance
Field test for ataxia: Ask the trekker to walk heel-to-toe in a straight line. If they cannot do this, treat it as a severe symptom and arrange descent.
How to Prevent Altitude Sickness: Overview
The single most effective prevention is controlled, gradual ascent. No supplement, food, or preparation can replace the body’s need for time to acclimatise. The following principles apply across all high-altitude treks:
- Ascend gradually. Above 3,000 m, limit sleeping altitude gain to 300–500 m per night. This is the most consistently supported guideline in wilderness medicine.
- Climb high, sleep low. Day hikes to higher elevations, followed by descending to sleep at lower altitudes, accelerate acclimatisation. This principle is built into most well-designed Himalayan itineraries.
- Build in acclimatisation days. Rest days at key elevations, like Namche Bazaar (3,440 m) and Dingboche (4,360 m) on the EBC route, are not optional padding. Skipping them significantly increases AMS risk.
- Stay hydrated. Aim for 3–4 litres of water per day at altitude. Dehydration worsens AMS symptoms and is common due to increased respiratory water loss in dry mountain air.
- Avoid alcohol and sedatives. Both suppress respiratory drive during sleep, impairing the body’s natural ventilatory response to altitude. This effect is most significant in the first 48–72 hours at a new elevation.
- Do not ascend with symptoms. If any AMS symptoms are present, rest at the current altitude until they fully resolve. This rule applies regardless of itinerary pressures.
For a full prevention guide, including acclimatisation schedules, training recommendations, and the role of medications, see our complete altitude sickness prevention guide.
Treatment of Altitude Sickness
Treatment depends on severity. The underlying principle across all levels is the same: do not ascend until symptoms resolve, and descend if they worsen or fail to improve.
Mild AMS: Rest at the current altitude. Do not ascend. Most mild AMS resolves within 12–48 hours with adequate rest and hydration. Ibuprofen (commonly used at 400 mg) has demonstrated efficacy for headache relief in clinical studies but does not treat the underlying cause.
Moderate AMS: Stop all ascent. If symptoms do not improve after 24 hours of rest, descend 300–500 m. Even a modest descent often produces rapid symptom relief. Supplemental oxygen, where available, can provide temporary relief.
Severe AMS, HAPE, or HACE: Descent is the only definitive treatment. There is no alternative. Descend immediately (at minimum 300–500 m), more if logistics allow
- Do not wait for morning or better weather if the trekker’s condition is deteriorating
- Supplemental oxygen reduces symptoms during descent but does not replace descent
- Portable hyperbaric chambers (e.g., Gamow bags) can simulate descent in emergencies and are carried by rescue teams on major Himalayan routes
Do not self-medicate based on information in this guide. Always consult a physician before your trek.
Medication options, including acetazolamide (Diamox) and dexamethasone, are covered in detail in our medication guide.
Natural Remedies: What the Evidence Says
Various foods and supplements are cited as altitude sickness aids, particularly in Himalayan and Andean cultures. The evidence for most is limited, and none replace acclimatisation.
- Ginger: some evidence for reducing nausea associated with AMS, but no demonstrated effect on core AMS progression
- Garlic: traditional use in Himalayan communities; no robust clinical evidence for altitude illness prevention
- High-carbohydrate diet: Carbohydrates require less oxygen to metabolise than fats or proteins, which may provide a marginal support for energy production at altitude. The effect is modest but supported by general physiology.
- Coca leaves / tea: widely used in South American high-altitude communities; evidence is anecdotal, and use is culturally and legally context-specific
Hydration, adequate sleep, and a conservative ascent profile remain the only interventions with consistent evidence.
Helicopter Evacuation Considerations
On major trekking routes in Nepal, helicopter evacuation is available in clear weather conditions. However:
- Flights depend on visibility and wind
- Patients may need to be moved to a landing zone
- Insurance verification or payment guarantee is required before dispatch
Remote circuits such as Manaslu or Dhaulagiri may involve staged evacuation due to terrain and weather constraints.
Evacuation is a logistical process, not an instant solution. Early decision-making significantly improves outcomes.
The Safety Hierarchy
Altitude emergency management follows a clear progression:
- Stop ascent
- Rest and reassess
- Descend if symptoms persist
- Evacuate if severe symptoms develop
When uncertain, descend. Altitude illness responds to elevation loss. Delay increases risk. A well-planned trek with built-in acclimatisation, experienced leadership, and a defined evacuation protocol reduces severe altitude complications from likely to unlikely.
Altitude Sickness on Popular Himalayan Treks
Nepal’s, Tibet’s, and Bhutan’s major trekking routes all pass through significant altitude bands. Risk profiles differ by route based on maximum elevation, rate of ascent, and availability of acclimatisation days.
| Trek or Region | Maximum Elevation (m) | Maximum Sleeping Altitude (m) | AMS Risk Level | Critical Acclimatisation Points | Key High-Altitude points | Route Specific Challenges |
| Everest Base Camp (Nepal) | 5,545 m | 5,364 m | Very High | Namche Bazaar (3,440 m), Dingboche (4,360 m) | Kala Patthar (5,545 m), Everest View Hotel (3,880 m) |
|
| Dhaulagiri Circuit (Nepal) | 5,360 m | 5,050 m | Very High | Italian Base Camp (3,660 m), Glacier Camp (4,200 m), Dhaulagiri Base Camp (4,740 m) | French Pass (5,360 m), Dhampus Pass (5,240 m) |
|
| Snowman Trek (Bhutan) | 5,320 m | Above 4,000 m | Very High / Compounding | Not in source | Rinchen Zoe La (5,320 m) |
|
| Lhasa and Beyond (Tibet) | 5,200 m | 5,200 m | Very High | Lhasa (3,656 m) | Everest North Base Camp (5,200 m), Rongbuk Monastery (5,100 m) |
|
| Manaslu Circuit (Nepal) | 5,106 m | 5,100 m | High to Very High | Dharmasala (4,460 m) | Larkya La Pass (5,106 m) |
|
| Langtang Valley (Nepal) | 4,984 m | 3,870 m | Moderate to High | Kyanjin Gompa (3,870 m) | Tserko Ri viewpoint (4,984 m) |
|
| Jomolhari Trek (Bhutan) | 4,930 m | 4,080 m | Moderate to High | Jangothang (4,080 m) | Yalila Pass (4,930 m) |
|
| Annapurna Base Camp (Nepal) | 4,130 m | 4,130 m | Moderate to High | Chhomrong (2,170 m) | Annapurna Base Camp (4,130 m) |
|
In Conclusion…
Altitude sickness is the single most important health risk on any high-altitude trek. Thankfully, it is also highly manageable with the right knowledge and pacing. Understanding the symptoms, respecting gradual acclimatization, and responding early to warning signs are what allow trekkers to safely reach destinations like Everest Base Camp, Annapurna Base Camp, and beyond. The mountains reward patience, not speed. When you prioritize acclimatization over ambition, you dramatically increase both your safety and your chances of success.
Planning a high-altitude trek?
Explore our carefully designed itineraries with built-in acclimatisation days and expert guidance to help you trek safely and confidently👉 Check out the Trips